


35. An Avalanche of AEFIs
In Defence of Cautious Skepticism

Yellow Cards and VAERS
The Department of Health’s MHRA (Medicines and Healthcare products Regulatory Agency) professes to act ‘on behalf of the Ministers to protect and promote public health and patient safety, by ensuring that medicines and medical devices meet appropriate standards of safety, quality and efficacy’.
They run the Yellow Card scheme, which ‘collects and monitors information on suspected safety concerns or incidents involving: medicines, vaccines, medical devices, and e-cigarettes. The scheme relies on voluntary reporting of suspected safety concerns or incidents by healthcare professionals and members of the public (patients, users, or carers). The purpose of the scheme is to provide an early warning that the safety of a product may require further investigation.’
As we rolled out the novel Covid vaccines under EUA, I came across a number of potential adverse reactions in our patient group. I have recorded these and ‘Yellow-Carded’ significant AEFIs temporally correlated with Covid-19 vaccinations. This list very likely includes coincidental events, but I remain concerned about causality, particularly for temporally associated pro-thrombotic/pro-arrhythmic, vasculitic, neurological and immune-mediated conditions. Even if only a small number are true associations, it would still represent a concerning rate of ADRs for the size of our practice population.
When submitting a report, there is no way to know the cause. Nevertheless, we have a professional responsibility to report such episodes to the MHRA, more so when trialling new vaccine technology on an entire population. It is their job to determine causality.

VAERS (Vaccine Adverse Events Reporting System) is the US equivalent, national vaccine post-marketing safety surveillance program, administered by the FDA and CDC. Like the UK Yellow Card system, anyone can report to VAERS. Knowingly filing a false VAERS report is a violation of Federal law and punishable by fine and imprisonment.
There are clear benefits and limitations to passive voluntary surveillance notification systems open to both public self-reporting and to health professionals. The Yellow Card and VAERS online reporting systems have been described as cumbersome to use - both too are sensitive to medical and public opinion. On this subject, a pseudonymous senior government researcher/scientist who writes the Substack ‘Bartram’s Folly’, provides a compelling case that when medical professionals and the public are left to make the decision as to what is a genuine adverse event, bias leads to both over and under-reporting of potential reactions:
Despite the inherent deficiencies of the Yellow Card System, we could still see that very commonly reported ADRs calibrated qualitatively well with information we had received in February 2021 from the Oxford-AstraZeneca vaccine trials. In those trials, the most commonly reported reactions, after injection site tenderness/pain were:
Headache: 52.6% of trial participants
Fatigue: 53.1%
Myalgia: 44%
Malaise: 44.2%
Pyrexia/feverishness: 33.6%
Chills: 31.9%
Arthralgia: 26.4%
Nausea: 21.9%.
This also tallied with our post-vaccination experience in the workplace.
To illustrate the scale of under-reporting of common self-limiting reactions, it is evident that the majority of these ADRs were not formally ‘yellow-carded’. Of the first 49 million Oxford-AstraZeneca vaccine doses given, the proportion of Yellow Card notifications generated for:
Headache was 0.2% compared with 52.6% of trial participants experiencing headache (263 x under-reported)
Fatigue: 0.1% (531 x under-reported)
Myalgia: 0.06% (733 x under-reported)
Pyrexia/feverishness: 0.1% (336 x under-reported)
Arthralgia: 0.05% (528 x under-reported)
Nausea: 0.9% (24 x under-reported)
Intuitively though, one would expect serious and unexpected medical events after vaccination to be reported proportionally more often than minor ones.
An Avalanche of AEFIs
FDA Director Dr. Peter Marks would later describe an unanticipated 'avalanche' of Adverse Event Reports after the COVID-19 Vaccines were released:
”We tried to be prepared for that but the avalanche of reports was tremendous.”
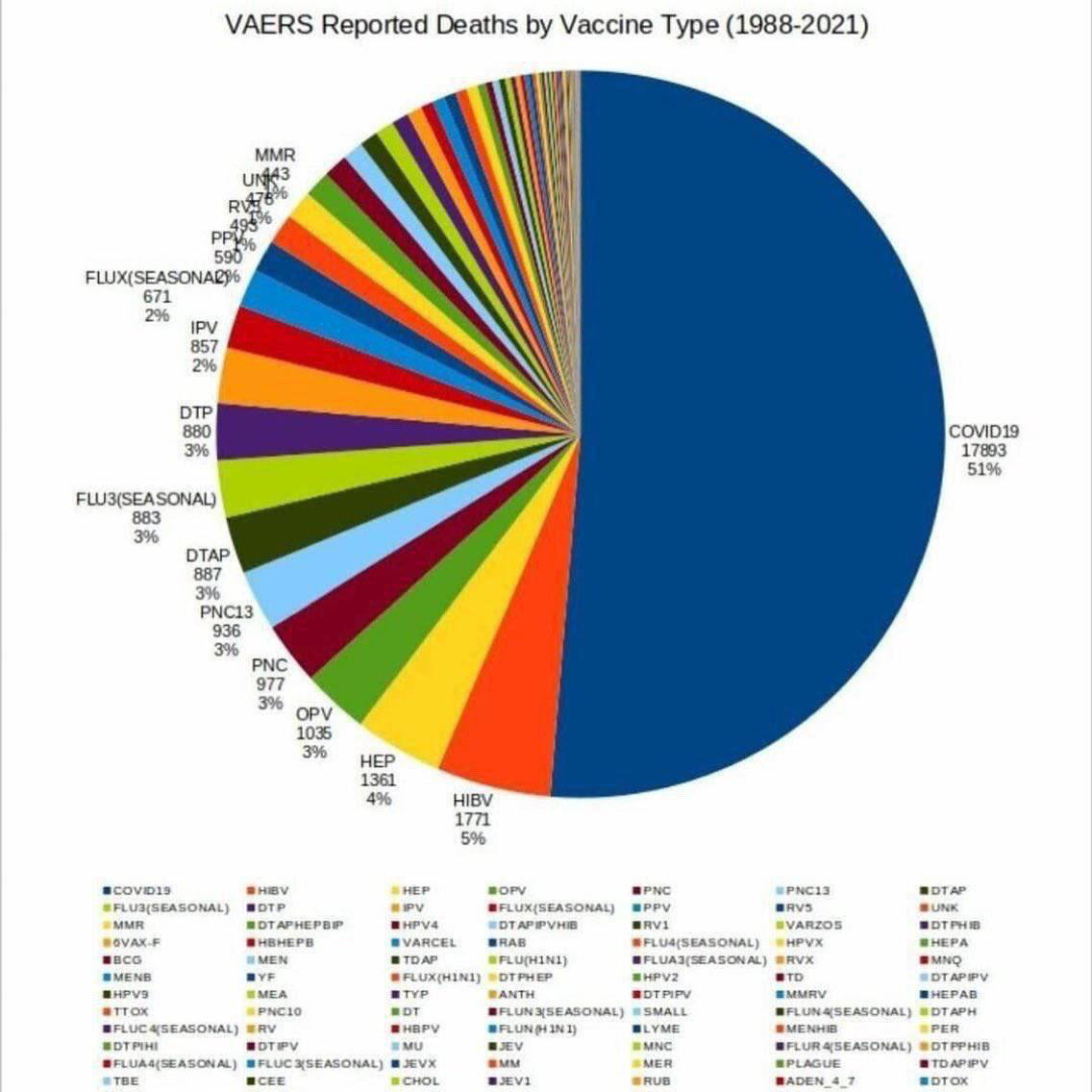
In fact, 2021 saw a 1540% increase in VAERS reports compared with the average for the last decade, and a higher VAERS associated mortality than with all vaccines combined in the last 20 years. Such a potential safety signal in VAERS naturally led to many questioning the safety of the new vaccines. This frustrated many doctors and academics who feared that the VAERS signal was being misinterpreted, abused and even ‘weaponised' by ‘anti-vaxxers’.
Yellow Card and VAERS data cannot of course be used to conclude causality, derive side effect rates or compare the safety profile of COVID-19 vaccines, as many factors can influence reporting. Unfortunately, these limitations have also given license to shut down discourse over the validity of VAERS and Yellow Card safety signals, often by those who are worried about fuelling vaccine hesitancy or who appear to give no credence to the overall significance of vaccine injury.
Kathleen Jamieson, founder of FactCheck.org and Director of the Annenberg Public Policy Centre - one of a long line of Gates-sponsored ‘philanthropic foundations’ - has published an opinion piece in JAMA Network suggesting that the VAERS system should be re-branded the “Vaccine Safety Sentinel” to help counter the tendency for the public to ‘misunderstand’ and ‘misinterpret’ the significance of VAERS signals.
In contrast to this depiction of VAERS as a highly sensitive safety sentinel system, a BMJ investigation in November 2023 raised concerns that the US’s VAERS isn’t operating as intended and signals are being missed. One reason for this is the overwhelming number of Covid-19 vaccine AEFI reports swamping the system (1.7 million out of 675 million doses administered). Unbelievably, despite reviewing nearly 20,000 preliminary reports of death, they had not acknowledged a single death linked to mRNA vaccines.
One in three reports subsequently disappeared from the publicly searchable database. The explanation for this is that the FDA and CDC maintain two separate VAERS databases: a public facing one containing initial reports; and a private, back end system containing all updates and corrections. This contrasts with the US’s equivalent system for non-vaccine drugs (FAERS) which is completely publicly accessible, including for updates. The reason for this difference in approach is not transparent.
The BMJ reports that physicians who filed serious VAERS reports say they were never contacted by clinical reviewers or were contacted only months later. One doctor reported the death of a 7 year old boy from cardiac arrest after Covid vaccination but this was never followed up by VAERS investigators. Another had reported the autopsy-verified death of a 15 year old boy from ‘stress cardiomyopathy’ just days after the boy’s second dose of the Pfizer-BioNTech Covid-19 vaccine. Unusually, in that case, the CDC contested the cause of death, a move which the reporting physician described as overstepping their role.
Uncritical Appraisal
History warns us that we should generally approach industry claims for drug safety and efficacy with cautious scepticism. It may have been considered reasonable to use such rapidly produced novel technology under EUA in high risk groups and the context of a ‘global health emergency’, but when it came to low risk adults and children, whose risk from infection was always low, extreme caution should have been exercised.
2020, however, saw a rapid roll-out of drugs under conditions of media-driven panic. The medical profession had been inculcated to uncritically accept and repeat assertions of the novel Covid-19 vaccines as ‘incredibly safe, highly effective’, with serious harms ‘very very rare’, and this without any experience of their real world effectiveness.
A seemingly dependent health service took industry claims on trust, without access to full trial data, in the knowledge that such data will be suppressed for years. Reports of vaccine injuries have often been censored, labelled as misinformation or received less media attention than stories of adverse outcomes from Covid-19 infection. When the subject of potential vaccine injury has been raised, we have often seen a reflex denial of causation, downplaying of any signals of risk, highlighting the higher risk from Covid-19 and affirmation of the overwhelming safety of these vaccines.
That we have been witnessing this same behaviour right from the point of vaccine roll-out, should raise questions about the objectivity of a profession who themselves bodily committed to the vaccines in December 2020, a time when safety data was limited to industry published data.
Media talking heads, like This Morning’s Dr Sarah Kayat, made early bold claims for vaccine efficacy:
‘After 12 days from the first vaccination of the Oxford-AstraZeneca vaccine, you are 100% effective against hospitalisation and death’ (sic).
Ofcom received 156 complaints about the factual basis of GP Dr Kayat’s comments, as viewers pointed out, ‘there is no possible way this claim can legitimately be made’.
More concerning were similarly wild claims made for vaccine safety. In a BBC Newsround interview on 10 June 2021, Scottish Government Adviser Professor Devi Sridhar informed UK 12-15 year olds that
“the vaccine is 100% safe for children”.
Following complaints to the regulator, this ‘100% safety’ claim was removed from the transcribed interview, which had already been broadcast to the nation’s children. The original recording archived by CitizenJournos can still be viewed here.
Rather than parroting ‘the vaccines are safe’, the most we could ever truthfully have said was that from the data that had been made available to us, we were not yet aware of any significant short-or long-term safety concerns.
As it would transpire, they weren’t in fact safe for all people and the following series of posts will attempt to examine how potential safety signals could be obscured.
Thanks for your response :) Re mortality data - as we know, we have significant excess deaths in UK (whether attributable to the jabs and/or other measures implemented, I know not at this point ). I do wonder about length of time for jab injuries to manifest given the mechanisms they appear to initiate? Might it be the case that numbers of deaths might not be recognised as jab-related should they occur months/years later? I'm aware that Peter Doshi, having looked at the trial data, cites SAEs generally as approx. 1-800. I agree that we need to know or at least be making stringent efforts to do so. The Scottish Inquiry seems to be asking some of the right questions (sadly and frustratingly the UK inquiry appears, to date, not to be asking relevant questions). What is certain, is that the damage done by the policy response to whatever was going on will resonate through generations.
The 'safe and effective' mantra has proved the jabs to be anything but. I am now of the opinion that there was no actual pandemic (as per Denis Rancourt's data analysis, which appears compelling) and thus there was never any need whatsoever for the nonsensical measures (including, and most especially, the 'vaccines') that were implemented. It has always puzzled me that MHRA received significant funding to 'beef up' the YCS/data reporting in 2019 (I believe) and yet, is now less than transparent in reporting data collected to the public. Link to a short clip where DR outlines his findings. https://twitter.com/denisrancourt/status/1740872581987635278